Accuracy in Calprotectin Testing
Method Comparison of Four Automated Devices
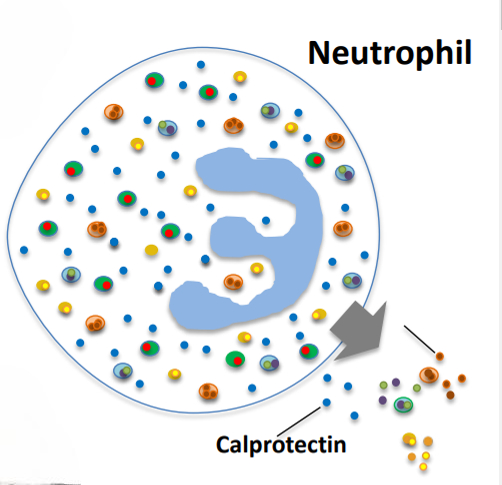
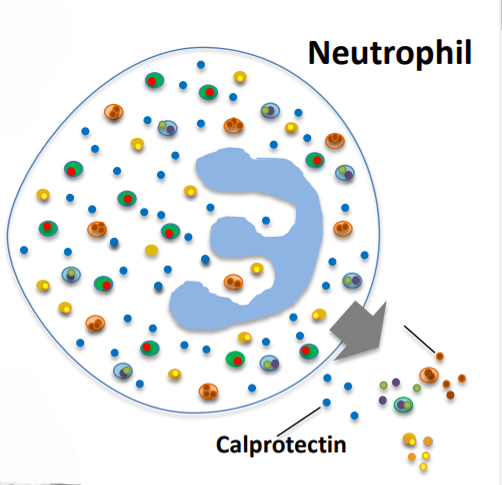
Though colonoscopy remains the definitive test for a positive diagnosis of Inflammatory Bowel Disease (IBD), the American College of Gastroenterology Task Force determined in 2010 that “routine colonic imaging is not recommended in patients younger than 50 years of age with typical IBS [Irritable Bowel Syndrome] symptoms and no alarm features.”1 Due to overlapping symptoms in IBD, IBS and other gastroenterological disorders and increasing wait times for endoscopic testing, fecal calprotectin levels are increasingly being used to noninvasively stratify patients presenting symptoms of IBD and IBS before recommending a colonoscopy.2
In addition to the use of fecal calprotectin in the initial diagnosis of IBD, the American Gastroenterological Association is now recommending calprotectin testing in conjunction with other biomarkers, clinical symptoms, and endoscopic evaluation as part of a comprehensive treatment monitoring program for both Crohn’s disease and ulcerative colitis.3,4
Accuracy of Calprotectin Tests
Differences in antibody affinity and specificity, optimization for performance in a stool matrix, and stringency of batch release testing can affect the accuracy and reproducibility of stoolbased diagnostic tests from one vendor to another. Clinical specificity and sensitivity reported to the FDA for several automated calprotectin tests reveals high variability in clinical specificity in the diagnosis of IBD, with false positives as high as 14 out of 100 and 26 out of 100 for some tests (see Table 1 below).
| Assay | ALPCO IT | Diasorin CLIA | Inova CLIA | Buhlmann IT |
|---|---|---|---|---|
| Clinical Sensitivity | 90.5% | 88.2% | 89.5% | 91.1% |
| Clinical Specificity | 93.4% | 90.6% | 86.1% | 74.3% |
| Manufacturer Cut-Off | 50 μg/g | 120 μg/g | 120 μg/g | 80 μg/g |
Table 1: Published clinical specificity and sensitivity from manufacturer FDA 510(k) submissions.
Methodology
While the comparison of published clinical sensitivity and specificity provides some indication as to competitive performance, we sought to evaluate all four calprotectin testing platforms using a single set of stool samples for a more direct comparison of clinical performance.
In the recent study, a representative set of 20 raw stool samples, including positive and negative samples based on colonoscopy, were evaluated in all four platforms. The Diasorin Liaison® CLIA assay, the Inova QUANTA Flash® CLIA assay, and the Buhlmann fCAL® Turbo immunoturbidimetric (IT) assay were performed at three different clinical sites and compared with results on ALPCO’s immunoturbidimetric assay. Stool extracts were prepared according to manufacturer’s instructions using the manufacturer recommended device and extraction buffer and testing was performed according to each manufacturer’s instructions for use.
Results
Results for all 4 platforms along with the accompanying clinical diagnoses are reported for each sample below (see Table 2). Results above each manufacturer’s recommended cut-off and IBD diagnoses are displayed in red. Results below the cut-offs and non-IBD diagnoses are displayed in green. Per manufacturer’s instructions, samples reading in the indeterminate or “grey” zone were reported as negative for Diasorin and Inova and reported as positive for ALPCO and Buhlmann.
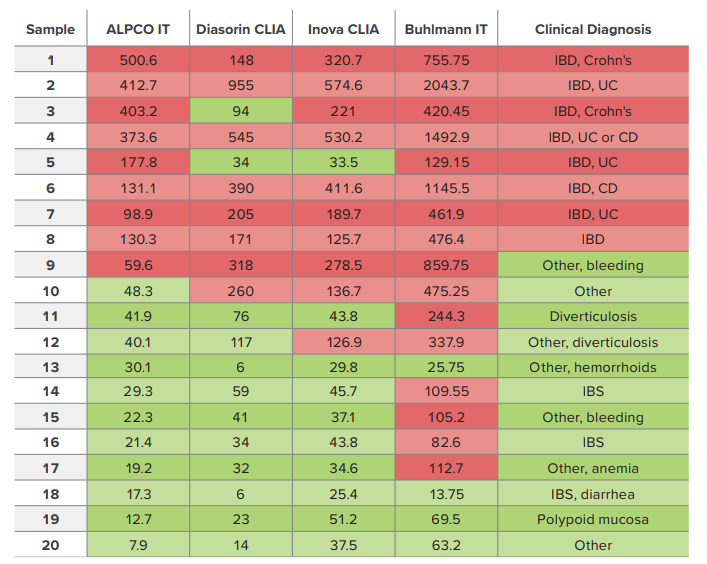
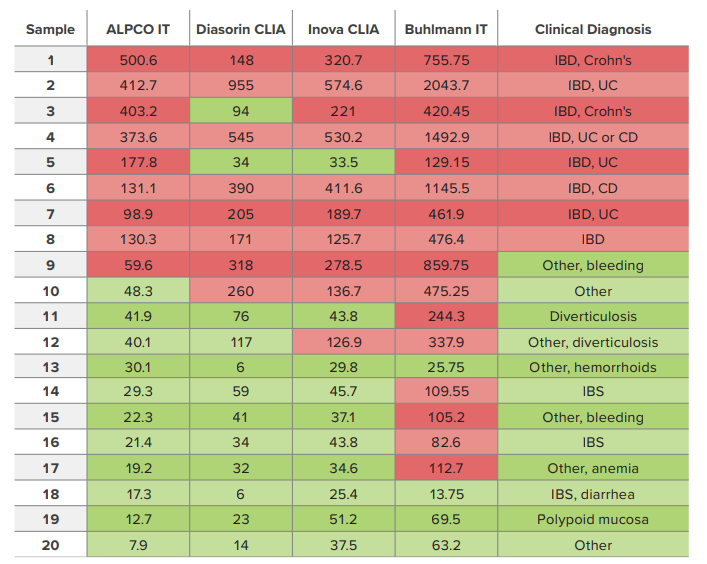
Table 2: Calprotectin results (in µg/g) from a recent 20-sample study. Mean results are reported for samples tested in duplicate.
Results for this small study trended similarly to the original 510(k) submissions, with clinical accuracy varying quite significantly from one manufacturer to another. Table 3 lists the number of false negatives per 8 clinically positive samples and false positives per 12 clinically negative samples for each assay. Clinical accuracy for diagnosis of IBD ranged from 95% for the ALPCO test, to 80% for the Diasorin and Inova assays, and 60% for the Buhlmann assay.
| ALPCO IT | Diasorin CLIA | Inova CLIA | Buhlmann IT | |
|---|---|---|---|---|
| Manufacturer Cut-Off | 50 μg/g | 120 μg/g | 120 μg/g | 80 μg/g |
| False Negative | 0/8 | 2/8 | 1/8 | 0/8 |
| False Positive | 1/12 | 2/12 | 3/12 | 8/12 |
| % Accuracy | 95% | 80% | 80% | 60% |
Table 3: False negatives, false positives, and % accuracy for 20 samples tested in each assay.
Conclusion
Laboratory directors are under increasing pressure to improve profitability through cost-cutting efficiencies and menu expansion. Automated, random access solutions including immunoturbidimetric and CLIA assays can reduce hands-on time (and labor costs), increase throughput (and testing capacity), reduce non-reportables (and reagent costs), and reduce operator-to-operator and usern errors (and costly re-tests). At the same time, clinicians continue to expect fast, accurate results. ALPCO’s automated turbidimetric solution for calprotectin testing offers enhanced efficiency without compromising clinical sensitivity or specificity. Clinicians can prioritize endoscopic evaluation for the patients that need it most and quickly put IBS patients on the right treatment path.
1 - Chey WD, et al. (2010). The Yield of Colonoscopy in Patients With Non-Constipated Irritable Bowel Syndrome: Results From a Prospective, Controlled US Trial, Am J Gastroenterol., 105:4, 859-865.
2 - Manz, M., et al. (2012). Value of fecal calprotectin in the evaluation of patients with abdominal discomfort: an observational study, BMC Gastroenterology, 12:5.
3 - Ananthakrishnan, A. N., et al. (2023). AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Crohn’s Disease. Gastroenterology. 165:1367-1399
4 - Singh, S. et al. (2023). AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Ulcerative Colitis. Gastroenterology. 164:344-372.