Researching Therapeutic Drug Monitoring for IBD
Multiple classes of biologics are available for the treatment of inflammation associated with inflammatory bowel disease (IBD) which ultimately improves the quality of life for patients. However, many challenges are associated with using biologics to treat IBD such as immunogenetic reactions and the rising cost of treatment1-4. These challenges are driving the need for more personalized and cost-effective approaches to IBD care5,6. Researching therapeutic drug monitoring for IBD biologics can increase the understanding of immunogenicity, assist with developing tools for personalized treatment algorithms, and lead to improved cost savings for patients and healthcare providers5-8. Furthermore, assays can assist in developing a therapeutic drug monitoring process for IBD biologics9,10.
What is Therapeutic Drug Monitoring?
Therapeutic drug monitoring (TDM) is a process utilized by healthcare providers to optimize treatment regimens for drugs such as antibiotics and immunosuppressants which allow for maximum efficacy and safety8. TDM provides insight into a drug’s circulating concentration and assists in maintaining a target therapeutic window8. Therefore avoiding low and ineffective doses as well as high and toxic doses8. Due to the large number of factors that influence drug response to IBD biologics such as immunogenicity, generating a clear path of therapeutic drug monitoring for IBD care is challenging5,7. However, gastroenterologists (GIs) and scientists are working to develop methodologies in order to apply TDM to the different classes of IBD biologics6,8,11.
Researching Therapeutic Drug Monitoring for IBD
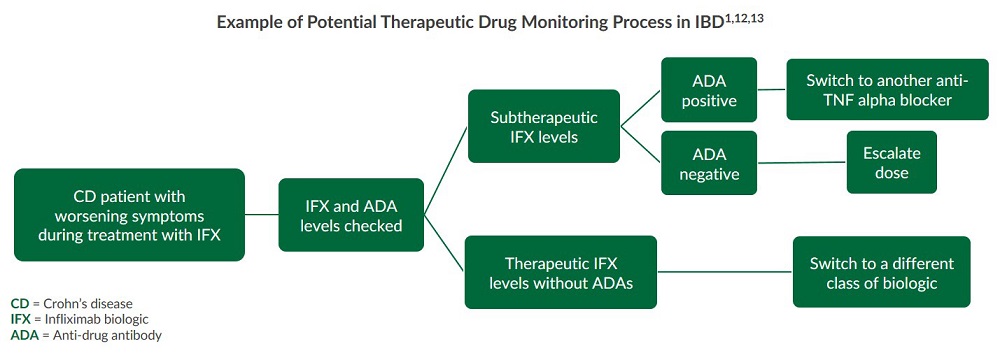
Without a clear understanding of how the body is reacting to a given IBD biologic, it is difficult to determine and overcome the root cause of primary non-response (PNR) and loss of response (LOR)5. Dose escalation and/or switching to another biologic are the suggested next steps when PNR or LOR occur1,12,13. Research indicates that therapeutic drug monitoring of drug and anti-drug antibody (ADA) levels during treatment can improve care by providing:Insight into PNR and LOR6,11
-
Determination of the appropriate biologic6,11
-
Dose and schedule optimization6,11
-
Improved clinical outcomes6,11
The following chart represents an example of a therapeutic drug monitoring process that can be used to research IBD and the immunogenicity of biologics:
Additionally, this video from the Gastrointestinal Society12 further outlines details around the concept of therapeutic drug monitoring for IBD, as well as how it can be used to help support IBD healthcare.
Building Research in IBD Globally
The Building Research in IBD Globally (BRIDGe) group has focused on developing a process to address resistance and loss of response to different TNF-alpha blocker biologics14. Formed in 2005, BRIDGe is a collaboration of 13 board-certified gastroenterologists with expertise in inflammatory bowel disease.
BRIDGe's Anti-TNF Optimizer
The BRIDGe GI’s have pursued challenging collaborative clinical research projects to help drive the future of IBD care. One such project was the creation of a web-based tool named the Anti-TNF Optimizer5. The Anti-TNF Optimizer was developed to help guide GI healthcare providers on how to respond to variations of TNF-alpha blocker drug concentration and anti-drug antibody levels in specific clinical scenarios. The tool was built for all approved TNF-alpha blocker therapies and is based on data collected from an extensive literature review on drug concentration and ADAs in patients with CD and UC. Numerous clinical scenarios were rated by GI professionals to generate the algorithm for the tool5. Users select answers to four questions focused around drug response, and the algorithm yields possible actions and recommendations for each individual IBD case:

BRIDGe anticipates the Anti-TNF Optimizer tool will be helpful when trying to make sense of the data generated from therapeutic drug monitoring in IBD5. This tool was developed as a research project and, therefore, is not intended nor recommended as a substitute for medical advice or treatment. More research needs to be completed to fully validate IBD therapeutic drug monitoring tools such as BRIDGe’s Anti-TNF Optimizer.
Potential Cost Savings of IBD Therapeutic Drug Monitoring
Research suggests that TDM of IBD biologics can provide cost savings benefits to patients and healthcare facilities6,11. A review of multiple studies using either patient data or simulations demonstrated a cost reduction between 28-34% for those whose healthcare providers utilized TDM in their IBD treatment strategy6. Additionally, simulation studies on large CD patient cohorts in the UK estimated a savings of $14,318.92 USD per patient five years after TDM was introduced6. Furthermore, these findings also indicated that utilizing TDM does not negatively impact the efficacy of the treatment6, further supporting the potential value of therapeutic drug monitoring in IBD.
Assays for Researching IBD Drug Response and Immunogenicity
Therapeutic drug monitoring assays can assist in researching drug response and immunogenicity through the measurement of both the drug and anti-drug antibody levels of different classes of IBD biologics 9,10. Such assays can ultimately aid in the development of TDM tools such as BRIDGe by providing the data needed to better understand:
- Drug trough levels10
- Target therapeutic window ranges10
- Effects of ADA formation10
In order to improve IBD care, gastroenterologists and scientists are investigating how to apply the principles of TDM to biologics treatments. Therapeutic drug monitoring for IBD biologics can offer healthcare providers deeper insight into drug response and immunogenicity, optimal treatment selection guidelines, and determining the right path to take when the drug is not working5,6,9,10. Furthermore, TDM for IBD may potentially result in beneficial cost savings for patients and healthcare providers6,11. Tools such as BRIDGe’s Anti-TNF Optimizer are being developed to guide the TDM process for IBD biologics5. Assays measuring the concentration of biologics and anti-drug antibodies can assist with IBD therapeutic drug monitoring research. However, collecting more data is necessary to develop additional tools and guidelines for each class of IBD biologics.
References
- Roda et al. (2016). Loss of Response to Anti-TNFs: Definition, Epidemiology, and Management. Clin Transl Gastroenterol. 2016 Jan;7(1):e135. doi:10.1038/ctg.2015.63. PMCID: PMC4737871.
- Smith et al. (2016). Unraveling the Effect of Immunogenicity on the PK/PD, Efficacy, and Safety of Therapeutic Proteins. Journal of Immunology Research. 2016;Article ID 2342187:9 pages. doi:10.1155/2016/2342187.
- Park et al. (2016). Health Insurance Paid Costs and Drivers of Costs for Patients With Crohn's Disease in the United States. The American Journal of Gastroenterology. January 2016;111:15-23. doi:10.1038/ajg.2015.207.
- Yu et al. (2018). Market share and costs of biologic therapies for inflammatory bowel disease in the USA. Aliment Pharmacol Ther. 2018 Feb;47(3):364-370. PMID: 29164650.
- Melmed et al. (2016). Appropriateness of Testing for Anti–Tumor Necrosis Factor Agent and Antibody Concentrations, and Interpretation of Results. Clinical Gastroenterology and Hepatology. 14(9):1302-1309. doi: http://www.cghjournal.org/article/S1542-3565(16)30195-1/fulltexth.
- Martelli et al. (2016). Cost-effectiveness of drug monitoring of anti-TNF therapy in inflammatory bowel disease and rheumatoid arthritis: A systematic review. J Gastroenterol. 2017 Jan;52(1):19-25. doi: 10.1007/s00535-016-1266-1. PMID: 27665099.
- Ben-Horin et al. (2015). Optimizing biologic treatment in IBD: Objective measures, but when, how and how often? BMC Gastroenterology. 2015;15:178. doi:10.1186/s12876-015-0408-x.
- Cheifetz. (2017). Overview of Therapeutic Drug Monitoring of Biologic Agents in Patients With Inflammatory Bowel Disease. Gastroenterol Hepatol (N Y). 2017 Sep;13(9):556–559. PMCID: PMC5635433.
- Vaughn et al. (2015). Biologic Concentration Testing in Inflammatory Bowel Disease. Inflamm Bowel Dis. 2015 Jun;21(6):1435–1442. PMCID: PMC4437804.
- Vermeire & Gils. (2013). Value of drug level testing and antibody assays in optimizing biological therapy. Frontline Gastroenterol. 2013 Jan;4(1):41–43. PMCID: PMC3533399.
- Kopylov et al. (2014). Therapeutic drug monitoring in inflammatory bowel disease. Ann Gastroenterol. 2014;27(4):304–312. PMCID: PMC4188926.
- GI Society. (2014). Therapeutic Drug Monitoring [Video]. GI Society. Inside Tract® Newsletter. 2014;189.
- Scott & Lichtenstien. (2014). Therapeutic Drug Monitoring of Anti-TNF Therapy in Inflammatory Bowel Disease. Curr Treat Options Gastroenterol. 2014 Mar;12(1):59-75. doi:10.1007/s11938-013-0004-5. PMCID: PMC4090075.
- BRIDGe. (2017). About the BRIDGe Group. BridgeIBD.com.